CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Annual Review of Criminology
Opioids and the Criminal
Justice System: New
Challenges Posed by the
Modern Opioid Epidemic
Jonathan P. Caulkins,
1,2
Anne Gould,
1
Bryce Pardo,
1
Peter Reuter,
2,3
and Bradley D. Stein
2,4,5
1
Heinz College, Carnegie Mellon University, Pittsburgh, Pennsylvania 15213, USA;
email: caulkins@andrew.cmu.edu
2
RAND Drug Policy Research Center, Santa Monica, California 90407, USA
3
Department of Criminology and Criminal Justice and School of Public Policy, University of
Maryland, College Park, Maryland 20742, USA
4
RAND Corporation, Pittsburgh, Pennsylvania 15213, USA
5
University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania 15213, USA
Annu. Rev. Criminol. 2021. 4:14.1–14.23
The Annual Review of Criminology is online at
criminol.annualreviews.org
https://doi.org/10.1146/annurev-criminol-061020-
125715
Copyright © 2021 by Annual Reviews.
All rights reserved
Keywords
heroin, opioids, drug policy, coerced treatment, drug enforcement
Abstract
The traditional US heroin market has transformed into a broader illegal opi-
oid market, dominated rst by prescription opioids (PO) and now also by
fentanyl and other synthetic opioids (FOSO). Understanding of opioid-use
disorder (OUD) has also transformed from being seen as a driver of crime
to a medical condition whose sufferers deserve treatment. This creates new
challenges and opportunities for the criminal justice system (CJS). Address-
ing inmates’ OUD is a core responsibility, including preventing overdose
after release. Treatment can be supported by diversion programs (e.g., drug
courts, among others) and by providing medication-assisted treatment in
prison, not only as a crime-control strategy but also because of ethical and
legal responsibilities to provide appropriate healthcare. The CJS also has
opportunities to alter supply that were not relevant in the past, including
deterring pill-mill doctors and disrupting web sites used to distribute FOSO.
.
CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
INTRODUCTION
Before the cocaine/crack epidemic of the 1980s and 1990s, heroin dominated the criminal justice
system’s (CJS) focus on illegal drugs. When President Johnson’s Crime Commission (Pres. Comm.
Law Enforc. Adm. Justice. 1967) wrote its landmark 1967 report The Challenge of Crime in a Free
Society, the chapter on drugs centered on heroin (Pardo & Reuter 2018).
Heroin had long been understood to cause crime, particularly property crime (e.g., Gandossy
et al. 1980, Preble & Casey 1969). The role of the CJS was to reduce crime, ergo it had to deal
with heroin. Tactics varied, including disrupting supply (e.g., the French Connection case of movie
fame) and reducing demand [the Nixon Administration’s embrace of Treatment Alternatives to
Street Crime (TASC) (Inciardi & McBride 1994) and rapidly expanding methadone provision]
(Musto 1999). But the focus was on reducing heroin use, in part for the public health benet but
importantly as a strategy for reducing property crime.
In the 1980s, cocaine, including crack, eclipsed heroin. Concern about the drug–crime con-
nection shifted to disorder and violence—particularly systemic violence associated with drug
distribution—and the policy response stressed border interdiction and source country control,
mandatory sentences, cracking down on street markets, and other policing innovations.
Times have changed again. Cocaine receded, with a startling and still largely unexplained 50%
decline in consumption between 2006 and 2010 (Caulkins et al. 2015). Whereas in 2005, cocaine
had by far the largest retail sales volume, by 2015 it may have fallen to fourth, after cannabis,
heroin, and methamphetamine (Midgette et al. 2019). However, recent historic increases in co-
caine production in Colombia may indicate a reversal of cocaine’s declining status (DEA 2019).
Today’s opioid crisis differs markedly from the traditional heroin problem. The problem draw-
ing the most attention now is not street crime but opioid overdose death and not just from heroin.
Deaths are greatest where illicit fentanyl is common, and most of those dying started their opioid-
using careers with prescription opioids (PO) rather than heroin (Cicero et al. 2014).
The shift is more subtle than just a multiplicity of opioids being available. For example,fentanyl
deaths are increasing as fast if not faster than opioid deaths increased in past drug crises. Yet it is
more a crisis of fentanyl poisonings than new drug use (Pardo et al. 2019b). Drug users are not
generally asking for fentanyl, at least not initially, and it does not spread primarily by word of
mouth among users. Its growth stems instead from drug dealers cutting their raw material costs
by substituting cheaper synthetic opioids for heroin.
Hence, it is now appropriate to review what is known about opioids and the CJS and chart fu-
ture research directions. This review is organized into two parts. The rst part focuses on opioid
use, including challenges, opportunities, and responsibilities for opioid users who come in con-
tact with the CJS. The second part explores how opioid supply chains today differ from those of
the past and the resulting implications for the CJS’s role in constraining supply, including both
limitations and new possibilities.
CRIMINAL JUSTICE SYSTEM AND OPIOID USERS
The Drug–Crime Connection
Criminologists have long grappled with the questions: Do drugs cause crime? If so, how much and
what kinds? The correlation is strong. Drug users are more likely to be criminals, and criminals
are more likely to use drugs than do otherwise similar people. The debate concerns the direction
and strength of the causal arrows between drugs and crime as well as how those arrows change
with the drugs’ legal status.
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Goldstein’s (1985) tripartite framework made a key distinction between (a) psychopharma-
cological crime that is caused by the psychopharmacological effects of drug use or withdrawal,
(b) economic-compulsive crime committed to obtain money to purchase drugs, and (c)systemic
crime associated with drug production, distribution, and sale.
Up through the 1970s, opioids—specically, heroin—were the focus because of their strong
association with economic-compulsive crime (Hammersley et al. 1989, Johnson et al. 1985), so
much so that the word narcotics was often used to mean all drugs. For example, heroin topped
the list of concerns for the President’s Crime Commission’s 1967 report, which observed that
heavy users were spending upward of $14 per day on it ($108 in 2020 dollars), whereas at the
time, cocaine was “not the major drug of abuse that it once was” (Pres. Comm. Law Enforc. Adm.
Justice. 1967, p. 213).
The levels of criminality reported by some heroin users were striking. Ball et al.’s (1982) classic
study conducted interviews over 11 years with a random sample of 243 heroin addicts (the standard
term at the time) selected from users identied or arrested by Baltimore police between 1952 and
1971. During periods of addiction, subjects had six times as many crime days per year as they
did during periods of abstinence. Although many of the crimes were just thefts, the volume was
startling: 248 crime days per year when addicted versus 41 per year when not addicted.
Ball et al.’s (1982) subjects were atypical. Their extraordinary rates of criminal activity are not
matched by all people with addiction, some of whom are not involved in nondrug crime at all.
Multiplying their very high offending rates by estimates of the total number of heroin users pro-
duced implausibly high estimates of the amounts of drug-related crime, but that implausibility did
not prevent such mythical numbers from causing alarm (see, e.g., Reuter 1984).
The nature of the drug–crime problem changed in the 1970s when the heroin epidemic stalled
(Agar & Schacht Reisinger 2002, Massing 2000) and 1980s when cocaine—including crack—
surged. That shifted concern to violence and disorder related to dealers and markets. Goldstein
et al.’s (1989) study of New York City homicides concluded that half were drug-related, with the
great majority related to cocaine and, in the language of Goldstein’s tripartite framework, most
were systemic crimes.
Cocaine-related violence inamed fears of the extent to which drugs drive crime, prompting
efforts to tamp down exaggerated fears. For example, Nordstrom & Dackis (2011) observed that
even though addiction may increase the frequency of criminal activity, it does not necessarily turn
nonviolent criminals into violent criminals. Likewise, Parker et al. (1998,p.295) argue strenuously
that alcohol, not illegal drugs,is most strongly connected to violence,andthat “evidence to support
a link between heroin and violence is virtually nonexistent.”
Efforts to combat the myth that all crime by drug users is drug-related can go too far, los-
ing track of the fact that use of expensive and addicting illegal drugs can substantially increase
an individual’s offending. For example, Parker et al.’s (1998) statement pertains primarily to psy-
chopharmacological, not systemic, crime and requires classifying economic-compulsive robberies
as a property, rather than violent, crime. Heroin users in the United States support a $30–$40 bil-
lion black market (Midgette et al. 2019) that generates considerable systemic violence in both the
United States and Mexico (Reuter 2009). Furthermore, Goldstein’s framework only encompasses
drugs as proximate causes of crime; there are myriad ways in which drug distribution, use, and
dependence also cause crime indirectly and over time.
For example, illegal drug dealing gives youth an incentive to acquire rearms, potentially trig-
gering an arms race among youth that makes all disputes more lethal (Blumstein & Cork 1996).
Were there no drug use or if drug markets were legally regulated and disputes resolved in court,
then there would be no illegal drug dealing and no such arms race; thus, drug use and the legal
www.annualreviews.org
•
Opioids and the Criminal Justice System .
CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
environment contribute in large part to violence, even if the person who pulls the trigger has not
used drugs. Likewise, drug use can interfere with school performance, and low educational at-
tainment can contribute to a broad array of adverse outcomes, including participation in crime
(Engberg & Morral 2006).
Still, the strongest evidence for a causal connection between opioids and crime pertains to
property crime. The Australian heroin drought provides one natural experiment. Australian data
show a long-term positive association between heroin use and robbery (Chilvers & Weatherburn
2003),and when heroin supplies suddenly dried up in early 2001,ratesof acquisitive crime changed
in expected ways. They rose initially (reecting a low short-term elasticity of demand) and then
went down as use adjusted downward to the higher prices (Degenhardt et al. 2005a,b; Smithson
et al. 2004). Likewise, the fact that evaluations of opioid treatment—a topic to which we turn
next—routinely nd that treatment reduces criminal offending is strong circumstantial evidence
for a causal effect.
The Effectiveness of Opioid-Use Disorder Treatment Generally
and for Criminal Offenders
Providing appropriate treatment to people with a substance-use disorder who are criminally active
is an effective way to reduce crime (Prendergast et al. 2002). Indeed, one of the early programs of
President Nixon’s Special Action Ofce for Drug Abuse Prevention was called TASC. Holloway
et al.’s (2006, p. 623) meta-analysis of 28 (mostly American) studies concludes that “drug treat-
ment is effective at reducing criminal behavior,” with treatment group’s odds of reoffending being
reduced by 29% or 36% depending on the model used.
Medication-assisted treatment for opioid-use disorder. The promise of treatment is even
greater for opioids than for other illicit drugs because a variety of effective pharmacotherapies
are available. The consistent nding is that medication for opioid-use disorder (MOUD) achieves
a very favorable cost:benet ratio, and in many evaluations reductions in criminality are a prin-
cipal benet. For example, Gerstein et al. (1994) reviewed treatment programs in California and
concluded that 42% of all the benets accruing to California residents in the year following entry
into a program came from reductions in crime and criminal justice costs.
The original and perhaps still most familiar medication is methadone, which, like heroin, is a
µ-opioid receptor agonist.However, it is low potency and longer acting, so it prevents the cravings
and associated harmful behaviors common in an individual with an opioid-use disorder (OUD),
enabling the lives of individuals receiving methadone treatment to be more stable on a variety of
levels, including employment and social functioning, despite the continued physical dependence
on a narcotic.
A common view in the literature is that medication treatment, including with legal PO ago-
nists such as methadone (and in some countries even heroin itself ) or partial agonists (notably,
buprenorphine) is the gold standard of care for treating OUD. There are not similarly effec-
tive or approved medication treatments for individuals with cocaine- or methamphetamine-use
disorders.
Opioid antagonists, such as injectable naltrexone (Vivitrol
®
) have also been shown to be ef-
fective in treating OUD among individuals who are willing to use one and remain adherent, but
many patients actively dislike Vivitrol
®
and rates of uptake are lower and rates of nonadherence
commonly higher than with some other medications (Lee et al. 2018). Furthermore, injectable
naltrexone does not appear to offer the same protection against overdose as do buprenorphine
and methadone (Jarvis et al. 2018). The evidence supporting counseling without medication is
less robust, and abstinence-oriented approaches are not clinically recommended.
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Methadone maintenance treatment (MMT) has been evaluated myriad times, including with
high-quality randomized controlled trials. Meta-analyses consistently nd that MMT improves
health and life outcomes and usually nd that MMT reduces criminality (e.g., Amato et al. 2005,
Marsch 1998), particularly drug and property crime. One exception is Mattick et al.’s (2009)
Cochrane review, which found MMT to be superior to a placebo at treatment retention and re-
ducing drug use but not necessarily at reducing criminality or mortality; the three studies reviewed
by Mattick et al. for this purpose were all very dated. It is also important to understand that treat-
ment rarely produces abstinence, and the benecial effects come despite low retention, high use
of other drugs during treatment, and high relapse rates post-treatment (Marsch 1998).
Treatment of prisoners. Although the literature on MOUD in the general population has a
clear takeaway (treatment works), the literature specically on OUD treatment for inmates is
more nuanced. Mitchell et al. (2012) provided a systematic review of 74 experimental and quasi-
experimental evaluations of incarceration-based treatment programs, divided into four categories:
therapeutic communities, group counseling, boot camps for drug offenders, and maintenance pro-
grams (like methadone). Therapeutic communities were found to reduce both criminal recidivism
and drug relapse, group counseling reduced recidivism but not relapse, maintenance programs did
the opposite, and boot camps performed badly on both outcomes.
The effect sizes observed by Mitchell et al. (2012) were modest but important. The odds ra-
tio for effects on recidivism translates into reducing recidivism rates from 35% to 29% (a 17%
reduction). The corresponding effect for drug relapse was slightly smaller (a 15% reduction) and
based on just 22 of the 74 studies that included drug-use outcome measures.
Hedrich et al.’s (2012) systematic review of 21 studies (six experimental) of prisoners receiving
opioid maintenance therapy reached broadly similar conclusions. Although there were clear effects
on drug use in prison and treatment retention post-release, effects on crime and reincarceration
were described as equivocal. Four of nine studies found lower rates of reincarceration, but ve
did not. One of four studies assessing effects on self-reported criminality found reductions, but
these did not persist past six months. Two others found effects that approached statistical signif-
icance. Stallwitz & Stöver (2007) are slightly more positive, suggesting that the mediocre effects
on nondrug crime may be improved with greater dosages and treatment duration.
Perhaps there is some divergence between evidence of the benecial outcomes of OUD treat-
ment for the general population and expected benets with respect to reduced offending resulting
from treating incarcerated individuals. Although MOUD among incarcerated individuals can re-
duce subsequent offending, therapeutic communities and post-release supervision can produce
even greater reductions (Holloway et al. 2006). One possible interpretation is that individuals
with OUD but few other life challenges may do ne on a simple maintenance drug, but those
with comorbid mental health challenges, lack of family support, and multiple other stressors may
need more and/or different interventions, and those entangled with the CJS may often be in the
latter situation. Nonetheless, the consensus in the literature is that MOUD has repeatedly been
shown to reduce opioid use and criminal offending, and that treatment is also effective when it is
provided in a criminal justice setting.
Ethical Concerns Related to Providing Treatment in a Criminal Justice Setting
Focusing treatment on high-rate criminal offenders may offer taxpayers the greatest return-on-
investment because of reductions in offending, but it can create ethical questions. Merely offering
treatment does not ensure that an individual will engage and remain in treatment, as many people
with OUD do not want treatment and others initiate but drop out. Given this, is it appropriate
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
for the CJS to incentivize or even coerce treatment of those under its supervision as part of, or in
lieu of, a prison sentence? And, if so, for which categories of offenders?
The answer may depend on particulars. Farabee et al. (1998) described a continuum of coer-
cion ranging from a simple recommendation to policies that involuntarily send inmates to prison
treatment programs. Klag et al. (2005) emphasized that there is a difference between compulsory
treatment and coerced treatment.
The ethical question is intertwined with the question of effectiveness. Doug Anglin, Mary-
Lynn Brecht, and colleagues argued in several highly cited studies that treatment is equally ef-
fective for both legally coerced and voluntarily admitted participants (Anglin et al. 1989, Brecht
et al. 1993). However, more recent reviews (Farabee et al. 1998, Klag et al. 2005) have noted that
the ndings are mixed. Uncertainty about effectiveness seems to stem in part from the lack of a
clear denition of what coercion entails and how motivation of an individual can be determined
for those in the control groups as well as those in a mandated treatment program. Through in-
terviews with 415 clients in a wide range of treatment modalities, Marlowe et al. (2001) assessed
the multidimensionality of the pressures and motivations that can impact an individual’s decision
to enter treatment and found that nearly all clients reported a combination of pressures (family
and/or employers as well as courts) to do so.
Even if coerced treatment works, there is also the question of whether it is ethical. Substance-
use disorders are recognized as behavioral health disorders and disabilities, and treatment is a form
of medical care. The UN Convention on the Rights of People with Disabilities states that forced
treatment must be abolished. However, all US states have provisions for involuntary treatment of
mental health problems for individuals at risk of hurting themselves or others, and protecting the
public from crime can be seen as a compelling health interest.
Some authors have addressed this ethical dilemma (e.g., D’Hotman et al. 2018). Concerns
raised include whether individuals with OUD are able to provide consent, potential abuses to
human rights, and the nature of the relationship between client and therapist (Werb et al. 2016).
Werb et al. (2016, p. 2) argue that, “given the potential for human rights abuses within compulsory
treatment settings, noncompulsory treatment modalities should be prioritized,” but Ludwig &
Peters (2014) counter that MOUD in correctional settings is ethically appropriate.
Others argue that it is unethical for the CJS to not provide treatment. The United Nations’
Basic Principles for the Treatment of Prisoners stipulates that “prisoners shall have access to
the health services available in the country without discrimination on the grounds of their le-
gal situation” (General Assembly Resolution 45/111). Failing to provide treatment—including
medication-assisted treatment—can be seen as violating this principle of equivalence; in the
United States, the Eighth Amendment, given the Supreme Court’s 1976 ruling in Estelle v. Gamble
(Linden et al. 2018, Wakeman 2017), states that deliberate indifference to serious medical needs
constitutes cruel and unusual punishment.
Addressing Opioid Use/Dependence of Inmates
The Bureau of Justice Statistics estimates in surveys conducted in 2007 and 2009 that 58% of
state prisoners and 63% of sentenced jail inmates met the DSM-IV criteria for drug dependence
or abuse and one in six had regularly used heroin (Bronson et al. 2017). Female inmates experi-
enced an even higher prevalence of drug-use disorder (69% in prison and 72% in jail). There-
fore, addressing inmates’ OUD is a core responsibility, not a special situation, and creates its own
opportunities and challenges. Below, we discuss four aspects: incarceration interrupting existing
treatment, provision of treatment in prison, reduction of overdoses following release from incar-
ceration, and incorporation of treatment into post-release supervision.
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Interrupting treatment by incarceration. Continuity of care is important for all chronic ill-
nesses, including OUD. Given their length, prison sentences create opportunities for the CJS to
provide treatment, but shorter jail stays can harm detainees by interrupting ongoing treatment—
and most of those harmed have not yet been convicted, with people entering jail more than 10 mil-
lion times annually in the United States (Zeng 2019).
Interrupting MOUD potentially makes medication treatment less appealing for criminally in-
volved people with OUD. One qualitative study of incarcerated individuals with OUD who had
methadone discontinued during incarceration indicated that the painful experience made them
reluctant to engage in methadone treatment again after release (Maradiaga et al. 2016).
Paradoxically, interrupting ongoing use during incarceration may also reduce tolerance,
thereby increasing vulnerability to overdose upon release. This possibility is illustrated in a
study by Binswanger et al. (2007). Examining death records for 30,000 inmates released from
Washington State prisons between 1999 and 2003, they found that in the two weeks after release
the mortality rate was 12.7 times that of the general population (adjusting for age, sex, and race).
Drug overdose was the leading cause of deaths among the former inmates in this period.
Providing treatment within prison. Treatment availability, particularly of MOUD, is limited in
most US jails and prisons (Nunn et al. 2009) and, if available, is often available only to certain
populations, such as pregnant women who had initiated MOUD prior to incarceration (Sufrin
et al. 2020).As a result,only approximately one-quarter of incarcerated individuals reported having
received drug treatment since they were incarcerated, with very few mentioning treatment with a
maintenance drug (Bronson et al. 2017).
There have been some efforts to promote treatment within the US CJS. For example, the 1994
Violent Crime Control and Law Enforcement Act provided funding. However, other countries do
better. Larney & Dolan (2009) nd that at least 29 countries had implemented Opioid Substitution
Treatment in prison as of January 2008, including most EU countries (Hedrich et al. 2012) and
Australia (e.g., Hall et al. 1993).
Providing treatment can strain already stretched correctional budgets, but in an ideal world
that transcended bureaucratic silos, stretched budgets should not be an impediment to treat-
ment. Warren et al. (2006) argue that treating inmates need not be more expensive than providing
methadone in a community setting ($3,200 per inmate per year in that study).
There are also implementation challenges, e.g., the rural location of many United States pris-
ons, which can make it harder to recruit and retain specialty staff. Distance from inmates’ counties
of residence can also interfere with continuity of care after release (Farabee et al. 1999). There are
also concerns about diversion from the patient to other inmates.
However, a greater challenge may be overcoming opposition to methadone and buprenorphine
on the grounds that they simply substitute one opioid with another and that drug-free treatment
is superior. For example, in commenting on Stein et al.’s (2020) study of detoxication, Nunes &
Shulman (2020) note that it is important to recognize that the preference for drug-free treatment
may be held by not only leadership and staff of in-patient or residential programs but also other
key stakeholders, including clinicians at out-patient treatment programs, family members, people
in recovery from addiction, policymakers, and patients themselves.
However, systemic change is possible. In July 2016, Rhode Island became the rst US state to
screen every individual who entered a prison or jail for OUD and offer all three forms of MOUD
(buprenorphine, methadone, and naltrexone) along with drug counseling. Early results have been
positive. Comparing the rst six months of 2016 to the rst six months of 2017, there was a 60.5%
reduction in mortality among individuals recently released from incarceration (Green et al. 2018).
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Providing naloxone upon release. Naloxone is a short-acting opioid antagonist effective in
counteracting opioid overdose–related central nervous system and respiratory depression (Boyer
2012, Sporer et al. 1996). Recent years have seen many efforts to increase access to naloxone, a
nonscheduled drug that can be obtained and used by nearly anyone, including those under CJS
supervision. There is a particular need to counter the spike in deaths for individuals with OUD
in the weeks following their release from prison, as noted above.
Relatively few CJS-based naloxone distribution programs have been evaluated; however,
McDonald & Strang (2016) completed a systematic review of studies of take-home naloxone pro-
grams. The 22 studies covered 15 locations in 4 European or North American countries and
included both community and prison sites. Their review found that these programs reduced over-
dose mortality for program participants and the surrounding communities.
Prisoners can benet from community-wide as well as inmate-specic policies. Scotland im-
plemented its National Naloxone Program (NNP) in January 2011 for all at-risk individuals, in
prison or not. In a pre–post study design, Bird et al. (2016) found a 20–36% reduction attributable
to the naloxone program in the number of opioid-related deaths in the rst month post-release
from prison.
Likewise, providing naloxone to one person may save another person. In England, Parmar
et al.’s (2017) randomized controlled trial of naloxone-on-release concluded earlier than planned
due to the release of information related to Scotland’s NNP, but initial results showed that two-
thirds of the individuals who received the naloxone were not the individuals to whom it had been
distributed.
Providing treatment to individuals under criminal justice system supervision in the com-
munity. The majority of the population under CJS supervision is in the community, not incarcer-
ated. Kelly et al. (2013) found that treatment is as effective for those on probation or parole as it is
for others. There has been interest in extended-release naltrexone for this population because an
injected dose is effective for one month (Springer et al. 2015). A Cochrane review of oral naltrex-
one (which is typically administered in a once-a -ay pill) found it was no better than a placebo with
respect to the number of participants who were reincarcerated (Minozzi et al.2011). However,two
subsequent studies (Lee et al. 2018, Tanum et al. 2017) of extended-release naltrexone concluded
that it was as effective as buprenorphine–naloxone with respect to maintaining abstinence in the
short term.
Alternatives to Incarceration
Rising rates of drug use, crime, and violence were dominant concerns in the latter part of the twen-
tieth century, but excessive rates of incarceration eclipsed them in the twenty-rst century (Mauer
2006, Travis et al. 2014). There are particularly severe consequences for racial/ethnic minorities,
which have been likened to a new form of Jim Crow segregation (Alexander 2011). Incarceration
of low-level drug offenders has been seen as a major culprit (e.g.,Drucker 2002),with grave doubts
that imprisonment reduces recidivism (Green & Winik 2010, Spohn & Holleran 2002). Although
some disagree with the Jim Crow metaphor (Forman 2012) and the idea that incarceration for
drug law violations in particular was a singular driver (Pfaff 2014, 2017), there is almost universal
desire to reduce incarceration, even among conservatives (Dagan & Teles 2012).
Conventional probation has long been seen as insufciently rigorous, leaving a paucity of op-
tions between probation and incarceration (Morris & Tonry 1991) and a hunger for better ways to
supervise drug-involved offenders in the community. For drug-involved offenders, if the crimes
were caused by drug use, then stopping drug use could rehabilitate the offender without relying
on incarceration for deterrence of incapacitation.
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
This led to several distinct efforts aimed at diverting arrested/convicted low-level drug-
involved offenders away from long-term incarceration, including drug courts, diversion policies
such as California’s Proposition 36, and swift, certain, and fair (SCF) approaches such as Hawaii’s
HOPE program.
Drug courts. Drug courts implement a highly personalized and coordinated strategy, including
integrating alcohol or drug treatment services into sentences for drug-using offenders and rely
on ongoing judicial interaction, local partnerships, and frequent monitoring of participants’ drug
use to avoid incarceration. Drug courts rely on highly certain, but not overly severe, punishments,
designed not as retribution but rather to motivate a change in behavior.
Drug courts were a reaction to the failures of conventional monitoring, which tended to be
sporadic and ineffectual. To describe those failings in caricature, probation ofcers might rou-
tinely test offenders under community supervision, but failed or skipped drug tests confronted
the ofcer with the unappealing choice of ignoring the violation or seeking revocation of proba-
tion, potentially resulting in extended incarceration. There was often little ability to use graduated
sanctions, or their threat, to respond to intermediate levels of noncompliance. By contrast, drug
court clients’ progress was monitored frequently by the judge who had the authority to immedi-
ately implement a wide range of responses to violations.
Drug courts were rst established in the United States in 1989 and expanded rapidly, with
more than 1,600 drug courts established in the rst 20 years (King & Pasquarella 2009). They had
undeniable appeal, offering less drug use, lower crime, and reduced incarceration. However, drug
courts were received more skeptically in the academic literature (Anderson 2001, Belenko 2001,
Goldkamp et al. 2001, Holloway et al. 2006). A 2009 review of their effectiveness at reducing in-
carceration, reoffending, and criminal justice costs produced mixed ndings (King & Pasquarella
2009), whereas Aos et al.’s (2006) meta-analysis of 57 studies estimated that drug court participa-
tion reduced crime by 8% relative to no treatment. However, “of great concern is the contention
that drug courts could be increasing the number of people arrested for drug crimes, instead of de-
creasing in the long-term the number of people processed in the criminal justice system. Research
has not yet focused on determining whether drug court participants would have ended up in the
criminal justice system if not for the drug court” (King & Pasquarella 2009, p. 19).
Another criticism is that relatively few of those currently incarcerated (whether in jail or prison)
would have been eligible to participate (Pollack et al. 2011). Each drug court has its own eligibility
requirements, often set by the presiding judge, but many require that the offender have no history
of violent crime, no prior felony conviction,no arrest for drug sale or trafcking, and no drug court
failures in the previous ve years. Some drug courts also have capacity constraints, e.g., from limits
on the judge’s time. A 2008 study determined that within an estimated population of 1,471,338
arrestees who are at risk of OUD and probably guilty, and therefore more likely to participate
in such a program, only 109,921 were eligible to appear before a drug court. Of those who were
eligible, only 55,365 (or 3.8% of the population that could benet from this type of program)
actually received drug court treatment (Bhati et al. 2008). Also, at least as of 2010, only about half
of drug courts offered MOUD to participants with OUD (Matusow et al. 2013).
Swift, certain, and fair. Mark Kleiman (2009) argues in his inuential book When Brute Force
Fails that consequences that are swift, certain, and fair (SCF) are the most effective in reducing
drug use and associated crime. SCF is the opposite of many current probation practices, in which
sanctions are delayed, unpredictable, and overly punitive.
The SCF concept is relevant to but not restricted to offenders with OUD. Perhaps its most
famous implementation pertained primarily to methamphetamine-involved offenders in Judge
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Alm’s Project HOPE (Hawaii Opportunity Probation with Enforcement). This program does not
require that participants partake in drug treatment but does require they abstain from drug use
as conrmed by frequent and random testing. If a participant tests positive, they are subject to
immediate and moderate sanctions, such as an overnight stay in jail. Unlike drug courts, only
those participants who have violations appear in front of a judge, making the approach cheaper
and easier to scale than drug courts.
Hawken & Kleiman’s (2009) initial evaluation found that HOPE reduced drug use,new crimes,
and incarceration both for the high-risk probationers included in the initial pilot program and
a randomized controlled trial of general population probationers. Later evaluations have been
less favorable. In a demonstration eld experiment of the HOPE program in four US counties
selected through a competitive process, among more than 1,500 probationers randomly assigned
to HOPE or probation as usual (PAU), Lattimore et al. (2016) found that HOPE/SCF enrollees
were no less likely to be rearrested, with the exception of drug-related arrests at one site. An
evaluation of a similar Delaware program also found no effect on recidivism (O’Connell et al.
2016), but Washington State’s program fared better (Hamilton et al. 2016). South Dakota’s 24/7
Sobriety is another SCF-type program, originally for repeat DUI offenders but later extended to
drug offenders, that has very favorable evaluation results (Kilmer et al. 2013, Nicosia et al. 2016).
Hawken (2018) argues that the conicting outcomes suggest that SCF can work, but imple-
mentation can be challenging [Lattimore et al. (2016) note mediocre achievement of the swift
part of the SCF formula] and suggested that it may not be appropriate for all offenders; e.g., the
Arkansas site involved primarily low-risk offenders for whom such close scrutiny may have been
unnecessary and counterproductive.
Treatment as diversion from incarceration. A variety of states implemented measures to divert
low-level drug offenders from prison, with California’s the most ambitious and most studied.
In 2000, California’s Proposition 36 altered the state’s sentencing law for rst and second low-
level drug law violations, requiring that all eligible individuals (approximately 50,000 per year) be
provided the option to seek probation and treatment rather than incarceration. Like drug courts,
participants remain within the CJS, but unlike drug courts they receive much less attention; fur-
thermore, incarceration for noncompliance is prohibited. Several other states, including Arizona,
Hawaii, Kansas, Maryland, and Washington, subsequently passed similar initiatives.
Proposition 36 increased the number of arrestees going to treatment and reduced the number
going to prison, saving taxpayers money (Longshore et al. 2006), but treatment completion rates
were low because there was little to compel continued participation. Proposition 36 did not use
the threat of incarceration to increase treatment participation as much as it used referral to treat-
ment as a backdoor way of reducing penalties. Hser et al. (2007) also raised the concern that even
though Proposition 36 increased treatment among those within its mandate, it may not have in-
creased treatment overall if it displaced voluntary clients to make room for Proposition 36 clients.
Proposition 36 expanded treatment capacity in the state, although mostly in an outpatient setting.
THE CRIMINAL JUSTICE SYSTEM AND OPIOID MARKETS
The opioid markets and problems of greatest concern in twenty-rst-century North America
differ fundamentally from those of the past. Heroin markets and use eclipsed morphine around
the turn of the twentieth century, grew sharply in the late 1960s, and were largely stable from
the mid-1970s through approximately 2000, with an aging cohort of established, dependent users
supplemented by only a modest inow of new users.
Two factors broke that stasis. One came from the medical community: vastly increased pre-
scribing of POs, starting during the mid-1990s (Kolodny et al. 2015). The second came from
. Caulkins et al.
CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
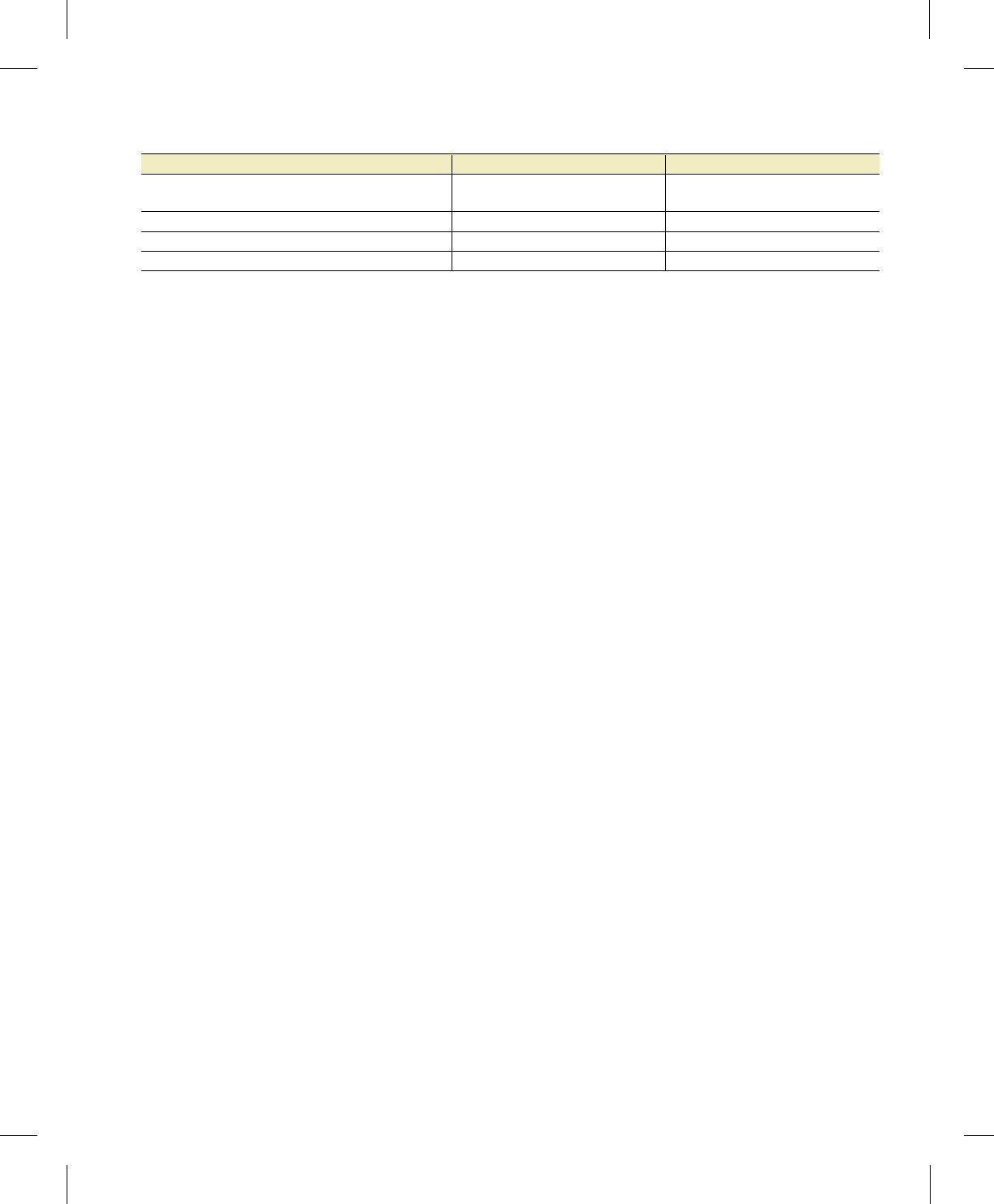
Table 1
Supply-side interventions by target sector and price chain link affected
Program Targeted sector Price affected
Eradication, alternative development, renery
destruction, precursor chemical control
Growing, production, and rening Export
Interdiction Smuggling Import minus export
Investigation High-level domestic trafcking Wholesale minus import
Street-level enforcement Retailing Retail minus wholesale
Data taken from Babor et al. (2018).
China, starting around 2014: black-market fentanyl and other synthetic opioids (FOSO) that are
vastly more potent than heroin (Pardo et al. 2019b). There is no consensus as to whether the rst
caused the second. Regardless of the causality, illegal opioid markets have been fundamentally al-
tered in ways that require new thinking about the capabilities and limitations of supply disruption
efforts.
The next three sections address this topic by (a) summarizing the conventional understanding
of supply control’s strengths and limitations vis a vis traditional markets, (b) distilling the essence
of what has changed, and (c) describing new opportunities for law enforcement to respond to
contemporary opioid supply.
Law Enforcement’s Capabilities and Limitations for Constraining
Traditional Heroin Markets
All heroin consumed in the United States is produced in other countries. Since about 2005,
Mexico has supplied almost all US heroin, but in previous eras the United States imported sub-
stantial quantities from Afghanistan (1980s), the Golden Triangle (1990s), and Colombia (1993–
2005). Mexico is a high-cost heroin producer, but production costs are much less important than
smuggling costs as a share of retail price; smuggling costs are lower for Mexico, sharing a long
border and a huge daily ow of commerce and trafc with the United States, than for any other
country.
There is a large literature on the consequences of efforts to suppress heroin markets. Longer
sentences, higher probability of arrest for a supply offense, and more seizures do not affect mea-
sures of availability, in particular, price. However, the research is not strong, because of both data
limitations and conceptual challenges (Pollack & Reuter 2014).
Enforcement against heroin should not be seen as a single intervention; rather,from production
to consumption, there may be up to ten transactions (Kilmer & Reuter 2009) spread across four
major links in the supply chain (production, international trafcking, wholesale distribution, and
retail sale), each with a specic kind of enforcement program,as reected in Table 1.Furthermore,
the effect of each type of enforcement shows up in a specic part of the price chain (Caulkins &
Reuter 2010, Reuter & Kleiman 1986). For example, interdiction of heroin smuggled into the
United States increases the risks and costs of smugglers. That increases what smugglers charge,
which is the difference between the price at which they buy heroin from the supplying country and
the price at which they sell it to the wholesale dealers in the United States. That specic increase
would then lead to a higher retail price.
Theory suggests that tougher enforcement should raise price and reduce consumption, yet
heroin prices fell steadily from 1980 to 2000, a period during which the risk of incarceration
apparently rose (Caulkins & Reuter 2010). The consistently negative ndings have generated
many efforts to explain this failure.
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Some have suggested that the labor supply curve may be very at with respect to enforcement
risk because it is easy to replace dealers at any level of the market. Retail sellers are recruited from
those with weak prospects in the legitimate labor market, and dealers at any level are happy to
move up the chain if there are vacancies. Incarcerating one dealer, therefore, merely creates an
opening for another individual willing to take the same risks for almost the same reward (e.g.,
Becker et al. 2006). Tough enforcement then just creates drug-selling labor force churn without
raising price. However, that only accounts for the failure of tough enforcement to increase price;
it does not explain the decline.
Another possibility is that the relevant labor pool grows over time because of the steadily wors-
ening economic prospects of those who continue to use heroin frequently. The longer the record
of incarceration and treatment an individual accumulates, the harder it is to obtain legal employ-
ment. That could have driven down the reservation wage of heroin-selling labor over the decades,
thus driving down prices. No current research has tested this or other potential explanations.
Mark Moore’s (1973) seminal article suggested that police could reduce consumption without
increasing prices by raising the search time (transaction costs) required to obtain the drug by
shutting down visible street markets. Mark Kleiman (1994) further elaborated on this idea, and
Rocheleau & Boyum (1994) found that it took about 50 minutes on average for a heroin user to
nd the drug after deciding to purchase it. Since the average number of purchases per week was
13, the purchase time (valued at minimum wage, which at the time was $4.25 per hour) was an
important contributor to the total cost of acquiring heroin, perhaps $50 on top of roughly $200
in cash. Yet substantially increasing search time cost seemed difcult, particularly after pagers and
cell phones made it easier for sellers and customers to nd each other, reducing the importance
of open-air markets and the associated violence and disorder.
Occasionally, a large heroin market experiences a long-term disruption. The Australian heroin
drought, discussed above, is a prominent instance. Quite suddenly, at the end of the year 2000,
the price of heroin in street markets in Australia rose sharply and purity declined; price and purity
did not return to the previous levels even ve years later. The result was a drastic reduction in
heroin consumption and a modest increase in use of other drugs, particularly methamphetamine,
as discussed above. There has been considerable disagreement at what caused this disruption. De-
genhardt and collaborators published several papers citing supply-side interventions as the most
plausible explanation (Degenhardt et al. 2005a,b,c). A large seizure and accompanying arrests/
convictions in Fiji were the most likely cause (Hawley 2002), but why the market took many years
to recover has been hard to pin down and is still left unanswered. The interpretation was com-
plicated by a simultaneous disruption in British Columbia, perhaps related to the same seizure,
which lasted only briey (Wood et al. 2006).
Later in 2001, the Taliban prohibited the growing of opium poppies, leading to substantial
price increases but not a true shortage of supply except perhaps in the Baltic states (Pardo et al.
2019b) because heroin and opium stocks were substantial (Paoli et al. 2009). A second year of
prohibition might have had a greater impact but the Taliban’s fall following the US-led overthrow
of the Taliban ended the prohibition, and it is unlikely that any other regime will be able to obtain
similar compliance with a poppy production ban.
What Makes Today’s Opioid Markets Different?
John Kaplan’s (1983) seminal book on heroin and public policy was aptly titled The Hardest Drug.
Yet by the turn of the twenty-rst century, the age-adjusted death rates for PO (technically, nat-
ural and semisynthetic opioids) already exceeded that of heroin (1.0 versus 0.7 per 100,000), and
PO deaths tripled in the rst decade of the twenty-rst century, whereas heroin deaths held
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
steady. Heroin deaths subsequently soared starting in 2010, reaching 4.9 per 100,000 in just six
years. Recently, deaths from synthetic opioids other than methadone—the category that includes
fentanyl—increased tenfold in just ve years, from 1.0 per 100,000 in 2013 to 9.9 per 100,000 in
2018.
All three waves—PO, heroin, and fentanyl—involve opioids and activate the same neurorecep-
tors (Compton et al. 2016); addiction to each is considered the same clinically, as an OUD and
not as separate drug-specic addictions. There are practical and psychological barriers separating
those who abuse only prescribed pharmaceuticals from those who purchase from illegal markets,
but trading down from the former to the latter is not uncommon (Mars et al. 2014), and once
that barrier has been crossed, people with OUD often shift their opioid-of-choice in response to
changing price, availability, and market conditions.
Many of those dying of heroin and fentanyl launched their opioid-using careers with PO.
Cicero et al. (2014) studied 2,797 people entering treatment for heroin dependence. For 80%
of those initiating heroin use in the 1960s, heroin was their rst opioid of abuse, whereas 75%
of more recent heroin initiates were introduced to opioids through prescription drugs. Like-
wise, Muhuri et al. (2013) found that 80% of those reporting recent heroin initiation in the Na-
tional Survey on Drug Use and Health (NSDUH) were prior users of nonmedical pain relievers
(NMPRs). NSDUH has serious limitations for studying heroin use, but the relative risk rates are
striking. Muhuri et al. (2013) estimate heroin initiation rates of only 0.02% per year for those not
using NMPRs, but 0.38% per year for those using NMPRs 1–29 times in the past year and 4.1%
per year for those using NMPRs 200–365 times per year.
Prescription opioid analgesics (a category that includes OxyContin, Vicodin,and Percocet) had
long been used to treat, particularly, acute pain and chronic pain from cancer and terminal condi-
tions and patients within medical facilities. The radical change in medical practice in the United
States and, to a lesser extent, Canada was to greatly expand the use of powerfully addictive opi-
oids for treating chronic (as opposed to acute) pain of a general nature (e.g., back pain as opposed
to cancer pain) with minimal medical oversight (at home versus in a hospital or nursing home).
Pharmaceutical companies promoted this change aggressively (Kolodny et al. 2015).
Prolonged use of opioids results in physiological dependence. The question is what proportion
of long-term patients misuse compulsively or in ways that are not medically approved. The answer
turned out to be much higher than boosters promised (Meier 2018). The low rates of addiction
among people who took opioids briey to treat acute pain did not translate into similarly low rates
among those who took opioids for chronic conditions.
Edlund et al. (2014) estimated how treating chronic noncancer pain increased the odds of
developing OUD as a function of dose (low, medium, or high) and duration (acute versus chronic).
Even at high doses, treating acute pain with opioids only tripled the risk of developing OUD. But
with chronic treatment, the odds ratios were 15, 29, and 122 for low, medium, and high doses,
respectively.
This can create a conict of interest between pharmaceutical companies’ prot motives and
the public health interest because one opioid-tolerant chronic pain patient taking six pills per day
generates more sales revenue than 100 acute pain patients with seven-day prescriptions for two
pills per day. Even though prescribing peaked around 2010, US-per-capita prescribing remains
many times that of other developed countries (Humphreys 2017).
The shift in prescribing, and the resulting oversupply and diversion of PO, created a new popu-
lation of individuals with OUD that was geographically and demographically different from those
whose heroin use persisted for prior decades. PO initiation affected all ages, and, in many cases,
the supply of PO favored not urban markets but rural and suburban areas, especially in states with
lax prescription policies (Cicero et al. 2014, Powell et al. 2020).
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
PO oversupply can directly stimulate black-market supply in a way that differs from past opioid
markets. Heroin users may have introduced others to heroin (contagious spread of demand) and
worked as retail sellers, but they never produced additional supply. With PO, users turning to
criminal activity (fraudulent diversion) are actually expanding black-market supply (contagious
spread of supply). Curtailing excessive prescribing can disrupt that positive feedback loop.
The pendulum began to swing back with new guidelines for prescribers (Dowell et al. 2016);
laws aimed at curbing unscrupulous pain management clinics, prescribers, and dispensers (Kuehn
2014); and federal promotion of abuse deterrents such as the reformulation of oxycodone. Some
of these measures coincided with a rise in heroin deaths (Alpert et al. 2018, Cicero et al. 2012,
Evans et al. 2019), with some individuals potentially trading down to cheaper and more accessible
heroin as a result of those regulations, whereas others might have transitioned simply because of
tolerance developed from prescription pain relievers (Mars et al. 2014).
The heroin threat was soon eclipsed by illegally manufactured FOSO. Although some modest
amount of fentanyl diversion has occurred since the 1990s, after the drug was formulated to treat
chronic and end-of-life pain (Poklis 1995), the vast majority of harms stemming from fentanyl
are due to illegally manufactured product often concealed in the supply of other drugs. FOSO
appeared in illegal markets as early as the late 1970s, but prior outbreaks were comparatively
short-lived and limited in their reach (Pardo et al. 2019b).
Today’s FOSO problem differs markedly from prior heroin or PO problems for several reasons.
First, fentanyl sells online in wholesale quantities for approximately 1% of the price of heroin
per morphine-equivalent dose (MED) (Pardo et al. 2019b). Second, FOSO are an ever-changing
family of chemicals, not just one molecule, complicating detection and interdiction efforts and
sowing confusion in markets. Fentanyl is approximately 30–50 times more potent than heroin,
whereas carfentanil may be 10,000 more potent, so the margin of error in dosing is very narrow
even in the rst case and minuscule in the second. Third, these drugs are often concealed in or sold
as traditional drugs of abuse. A little bit of fentanyl powder can be mixed into heroin to give it an
extra kick or pressed into counterfeit prescription tablets made to look like genuine medications.
The rise of FOSO was facilitated by a shift in production and the rise of e-commerce. Although
Mexican drug-trafcking organizations had briey entered into fentanyl production in 2005, only
more recently did they start to expand production in earnest (Felbab-Brown 2019).Semilegitimate
and under-regulated pharmaceutical and chemical companies in China appear to have started
synthesizing and distributing fentanyl and various precursor chemicals to buyers around the globe.
Chinese producers faced little regulatory scrutiny and could advertise online, offering to ship the
drugs by post or express consignment (O’Connor 2017). Buying FOSO online upends traditional
distribution patterns. Someone without a criminal record or history of drug trafcking could use
the internet to import ten grams of fentanyl, enough to be a small-time wholesaler, without ever
dealing with transnational criminals.
Some ways FOSO are sold to end-buyers are also new. Recently, most pills purchased from
street dealers were diverted from legal pharmaceutical supplies. Their sale was illegal, but the
product was pure and quality controlled. Now, many pills that look like PO are actually counter-
feits containing potent synthetic opioids that expose customers to a substantial risk of overdose.
Opportunities for the Criminal Justice System to Address Opioid Supply
in the Modern Era
The changes in the nature of the illegal opioid problem in the United States require changes in the
strategy and goals of the CJS response. Here, we provide insights about supply disruption aimed
at two distinct ows: PO and FOSO.
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Disrupting prescription opioid supply. Reducing oversupply and diversion of PO is primarily
a healthcare system responsibility. Diversion happens in myriad ways (Inciardi et al. 2007a) but
commonly within the context of a doctor–patient relationship in which the patient is sincere and
the doctor is at most naïve or careless but not knowingly promoting diversion. Consider opioid
prescribing from surgery—a condition that patients are unlikely to fake to obtain opioids. In 2016,
it produced 3.3 billion unused pills in the United States (QuintilesIMS Inst. 2017). At $20 per pill,
the potential black-market value of excess prescribing from just surgery matches or exceeds that
of the entire heroin market (Midgette et al. 2019).
Important strides have been made to reduce overprescribing, and Simeone (2017) detects large
declines in apparent cases of doctor shopping between 2008 and 2012 in a database of 11 billion
prescriptions. Nevertheless, addressing diversion of PO is a long-standing CJS responsibility, and
opioids are, or at least were, the most common subject of diversion investigations (Inciardi et al.
2007b). Efforts to address major theft and corruption from the pharmaceutical supply chain, such
as hijacking delivery trucks, appear to be largely successful inasmuch as the quantities diverted at
those levels seem to account for a modest share of PO misuse (Natl. Acad. Sci. Eng. Med. 2017).
Law enforcement has tread more lightly on the greyer area of corrupt physicians, e.g., those
operating so-called pill mills (Rigg et al. 2010), tending to rely on professional boards and other
forms of self-policing. Few physicians knowingly supply PO for misuse, but opioid prescribing is
highly skewed; Kiang et al. (2020) reported that the top 1% of prescribers accounted for 49% of
all opioid doses, so a few corrupt doctors can create signicant population-level harm.
Florida’s pill-mill crisis is the paradigmatic example. Rigg et al. (2012) interviewed 50 street
dealers of prescription drugs in South Florida. The dealers’ top three sources were visiting mul-
tiple pain clinics themselves with false claims about pain, sponsoring others to do so (one dealer
had a 25-person crew), and buying PO from indigent patients with prescriptions. Visiting a pain
clinic might cost the dealer $100 to $250 but net 200 pills each with a street value of $20. Florida’s
system was so porous that it inuenced supply throughout the southeastern United States (Rigg
et al. 2010).
In 2010, Florida nally responded by implementing tighter regulation of pill mills and a pre-
scription drug monitoring program and arresting physicians running pill mills, some of whom
were prosecuted for murder (Dyer 2015). The combination dramatically reduced diversion
(Surratt et al. 2014) and opioid-related overdose deaths (Gau & Brooke 2017, Surratt et al. 2014).
Kennedy-Hendricks et al. (2016) credit Florida’s laws against pill mills and their enforcement with
averting 1,029 deaths from PO overdose over a 34-month period, although Florida’s Prescription
Drug Monitoring Program also contributed to the declines (Delcher et al. 2015).
Florida’s experience highlights the limitations of physician self-regulation.Davis & Carr (2017)
identied 43 Florida physicians who faced criminal action for illegal prescribing of opioids be-
tween 2010 and 2015. Of the 25 who were convicted or pled guilty and who had their medical
license permanently revoked, only one lost the license before being convicted or pleading guilty,
suggesting that without law enforcement intervention the criminal activity would have continued.
Law enforcement can also address the willingness of some pharmaceutical companies to pi-
oneer new markets in ways that are criminal. The infamous example is PurduePharma, whose
marketing efforts contributed importantly to the sharp growth in opioid prescribing that began in
the 1990s (Kolodny et al. 2015). Purdue paid a $600 million ne after pleading guilty to criminal
misconduct and deceptive marketing of Oxycontin (Meier 2007). Yet that ne is small compared
to Oxycontin prots, reported at $4.7 billion just through 2006 (Armstrong 2019), so given the
number of deaths involved, incarceration may be a more effective and just deterrent.
In May 2019, multiple Insys Therapeutics executives were convicted on racketeering charges
for paying bribes to doctors to prescribe Subsys—their fentanyl-containing product—and for
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
falsifying statements to insurers about patients’ needs. Shortly afterward, the company led for
bankruptcy, and in January 2020, the company founder was sentenced to ve-and-a-half years in
prison. Insys’s head of sales and former CEO were also sentenced to prison. The head of sales
was quoted as saying that he knew that his actions were illegal and that the company was going
to get ned astronomical amounts, but he thought that the worst case for him personally was that
the government might go after his money. He “had no idea that criminally there would be con-
sequences” or that he might go to jail (Kuchler et al. 2020). Even if imprisonment only weakly
deters street-level heroin dealers with prior criminal records and few legal job prospects, it might
deter physicians operating pill mills and the owners and executives of pharmaceutical companies
who engage in criminal conduct regarding opioids.
Disrupting supply of illegally manufactured fentanyl and other synthetic opioids. The typ-
ical law enforcement response to drug threats is to investigate and dismantle trafcking networks
to reduce availability and raise prices. As noted above, this has resulted in some meaningful supply
disruptions for heroin and diverted prescription medications but little success at raising prices in
the long run.
FOSO are even more challenging. Their production does not rely on illicit crops that are
typically geographically constrained, as is the case of illicit opium poppies used in heroin manu-
facturing. All that is needed is access to inexpensive precursors and an understanding of chemical
synthesis. Large and under-regulated chemical and pharmaceutical sectors in Asia are unlikely to
comply in the short term and in some cases producers overseas may not be violating national laws.
Production costs are very low and shipping a kilogram of fentanyl from Asia through the postal
system may cost as little as $10 (Pardo et al. 2019a). Fentanyl and many other synthetic opioids
are orders of magnitude more potent than heroin, making them ideal for smuggling; as little as
10 grams of fentanyl could equate to nearly 10,000 doses. Therefore, fundamentally new ideas
and strategies are needed where fentanyl has become entrenched. Instead of focusing on raising
price and reducing availability, law enforcement may want to consider alternatives, like improving
market transparency and reducing the toxicity of the supply.
That said, there remain markets where fentanyl is still largely absent; at least through 2018,
FOSO were largely concentrated in states east of the Mississippi (Pardo et al. 2019b, Wilson et al.
2020). Markets where FOSO have not arrived may still benet from squelching supply, especially
before connections between buyers and sellers have developed. Doing so may save lives but will
require that law enforcement expand efforts to monitor local markets, perhaps through expanding
drug seizure analyses, partnering with social services that are in regular contact with drug users,
and piloting real-time surveillance systems such as wastewater testing.
Where markets are already swamped with FOSO, focused deterrence concepts developed to
respond to drug-related violence might be adapted. In essence, focused deterrence leverages a
full set of resources (both public and private) against the most egregious individuals while main-
taining a credible threat to the remaining actors to gain compliance (Kennedy 2009). The goal
is to nudge suppliers to act in ways that are less socially destructive. For example, the CJS might
send the message that it will aggressively pursue dealers that press FOSO into counterfeit tablets
made to look like prescription medications or mix them with stimulants. The concept would be
to investigate overdoses with the same sense of urgency as homicides, but focus punishment on
deterring future behavior, not punishing past actions. There may also be more creative options,
such as spoong websites that purport to sell FOSO but never fulll orders, sowing confusion
online and frustrating would-be importers.
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Implications for Research
Almost all literature reviews conclude more research is needed. This one is no different. The
justication is simple. The opioid problem of the twenty-rst century differs fundamentally from
the heroin problem of the twentieth century, which was arguably more harmful than the morphine
and opium problem of the nineteenth century. Whether or not past research on heroin and the
CJS is adequate is beside the point. Even if it were, it is a new century, with new problems.
This review identied two broad challenges for the CJS. The rst is recognizing that the moral,
legal, and practical responsibility of providing adequate healthcare to those in its charge includes
providing treatment and overdose prevention services to those with OUD. The stakes are high.
Many people with OUD encounter the CJS in any given year. That means the CJS has oppor-
tunities to intervene in ways that prevent many opioid overdose deaths. Myriad research-worthy
questions spin out from that basic moral imperative.
The second is that responding to the profound changes in opioid supply requires innovation.
Prospects for suppressing diversion of PO are fundamentally hopeful. The actors in that supply
chain are mostly licensed professionals; altering their behavior may require greater oversight and
investigation, but a little incarceration could go a long way. There are not nearly as many pharma-
ceutical executives as retail drug sellers, and the threat of incarceration may be a greater deterrent
to them.
The prospects for suppressing fentanyl supply are fundamentally discouraging, at least with
traditional approaches. Across all levels of government, criminal justice actors may need to move
beyond traditional goals of reducing availability and increasing price and instead embrace alter-
native goals of reducing overdose risk, e.g., by targeting suppliers who conceal FOSO in other
drugs or sell counterfeit tablets. Policing opioids may be better construed as being about public
safety, not law and order. Nevertheless, efforts aimed at treating OUD in criminally involved pop-
ulations presents a unique and life-saving opportunity to help stem the overdose risk of those who
are released.
When facing emerging challenges, law enforcement has proven its ability to innovate and adapt
(Weisburd & Braga 2006), but there are ample opportunities for researchers to help. The greatest
need now is not necessarily for new theories but for invention and evaluation of new programs and
practices. The potential reward for research is very high. Opioids killed almost 50,000 Americans
in 2018—quadruple the number of murders. The number of opioid deaths among people under
criminal justice supervision is not tracked but could well exceed the total number of homicides.
Yet homicide attracts considerably more attention from criminal justice researchers. It may well
be that the incremental benet in terms of potential lives saved per research project completed
is higher when studying new roles and opportunities for the CJS and opioids in the twenty-rst
century.
DISCLOSURE STATEMENT
The authors are not aware of any afliations, memberships, funding, or nancial holdings that
might be perceived as affecting the objectivity of this review.
LITERATURE CITED
Agar M, Schacht Reisinger H. 2002. A tale of two policies: the French connection, methadone, and heroin
epidemics. Cult. Med. Psychiatry 26(3):371–96
Alexander M. 2011. The new Jim Crow. Ohio St. J. Crim. L. 9:7
www.annualreviews.org
•
Opioids and the Criminal Justice System .
CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Alpert A, Powell D, Pacula RL. 2018. Supply-side drug policy in the presence of substitutes: evidence from
the introduction of abuse-deterrent opioids. Am. Econ. J. Econ. Policy. 10(4):1–35
Amato L, Davoli M, Perucci CA, Ferri M, Faggiano F, Mattick RP. 2005. An overview of systematic reviews
of the effectiveness of opiate maintenance therapies: available evidence to inform clinical practice and
research. J. Subst. Abuse Treat. 28(4):321–29
Anderson JF. 2001. What to do about “much ado” about drug courts? Int. J. Drug Policy 12(5):469–75
Anglin MD, Brecht ML, Maddahian E. 1989. Pretreatment characteristics and treatment performance of
legally coerced versus voluntary methadone maintenance admissions. Criminology 27(3):537–57
Aos S, Miller M, Drake E. 2006. Evidence-based public policy options to reduce future prison construction, criminal
justice costs, and crime rates. Rep., Wash. State Inst. Public Policy, Olympia. https://www.wsipp.wa.gov/
ReportFile/952/Wsipp_Evidence-Based-Public-Policy-Options-to-Reduce-Future-Prison-
Construction-Criminal-Justice-Costs-and-Crime-Rates_Full-Report.pdf
Armstrong D. 2019. Purdue’s Sackler embraced plan to conceal OxyContin’s strength from doctors, sealed de-
position shows. ProPublica. Feb. 21. https://www.propublica.org/article/richard-sackler-oxycontin-
oxycodone-strength-conceal-from-doctors-sealed-testimony
Babor TF, Caulkins JP, Edwards G, Fischer B, Foxcroft DR, et al. 2018. Drug Policy and the Public Good.New
York: Oxford Univ. Press. 2nd ed.
Ball JC, Rosen L, Flueck JA, Nurco DN. 1982. Lifetime criminality of heroin addicts in the United States.
J. Drug Issues. 12(3):225–39
Becker G, Murphy K, Grossman M. 2006. The market for illegal goods: the case of drugs. J. Political Econ.
114(1):38–60
Belenko S. 2001. Research on drug courts: a critical review, 2001 update. Natl. Cent. Addict. Subst. Abuse Rep.,
Columbia Univ., New York
Bhati AS, Roman JK, Chaln A. 2008. To treat or not to treat: evidence on the prospects of expanding treatment to
drug-involved offenders. Justice Policy Cent. Rep. NCJ 222908, Urban Inst., Washington, DC. https://
www.ncjrs.gov/pdfles1/nij/grants/222908.pdf
Binswanger IA, Stern MF, Deyo RA, Heagerty PJ, Cheadle A, et al. 2007. Release from prison: a high risk of
death for former inmates. New Engl. J. Med. 356(2):157–65
Bird SM, McAuley A, Perry S, Hunter C. 2016. Effectiveness of Scotland’s National Naloxone Programme
for reducing opioid-related deaths: a before (2006–10) versus after (2011–13) comparison. Addiction
111(5):883–91
Blumstein A, Cork D. 1996. Linking gun availability to youth gun violence. Law Contemp. Probl. 59(1):5–24
Boyer EW. 2012. Management of opioid analgesic overdose. N. Engl. J. Med. 367(2):146–55
Brecht ML, Anglin MD, Wang JC. 1993. Treatment effectiveness for legally coerced versus voluntary
methadone maintenance clients. Am. J. Drug Alcohol Abuse 19(1):89–106
Bronson J, Stroop J, Zimmer S, Berzofsky M. 2017. Drug use, dependence, and abuse among state prisoners and jail
inmates. 2007–2009. Bur. Justice Stat. Rep. NCJ 250546, Dep. Justice, Washington, DC. https://www.
bjs.gov/content/pub/pdf/dudaspji0709.pdf
Caulkins JP, Kilmer B, Reuter PH,Midgette G.2015.Cocaine’s fall and marijuana’s rise: questions and insights
based on new estimates of consumption and expenditures in US drug markets. Addiction 110(5):728–36
Caulkins JP, Reuter P. 2010. How drug enforcement affects drug prices. Crime Justice 39(1):213–71
Chilvers M, Weatherburn D. 2003. The impact of heroin dependence on long-term robbery trends. Crime Jus-
tice Bull. Rep. 79, NSW Bur. Crime Res. Stat., Sydney. https://pdfs.semanticscholar.org/dca2/
623fe7bb748f8ccd7d4c123f32d1794dc130.pdf
Cicero TJ,Ellis MS, Surratt HL. 2012. Effect of abuse-deterrent formulation of OxyContin. New Engl. J. Med.
367(2):187–89
Cicero TJ, Ellis MS, Surratt HL, Kurtz SP. 2014. The changing face of heroin use in the United States: a
retrospective analysis of the past 50 years. JAMA Psychiatry 71(7):821–26
Compton WM, Jones CM, Baldwin GT. 2016. Relationship between nonmedical prescription-opioid use and
heroin use. New Engl. J. Med. 374(2):154–63
Dagan D, Teles SM. 2012. The conservative war on prisons. Washington Monthly, Novemb./Dec. https://
washingtonmonthly.com/magazine/novdec-2012/the-conservative-war-on-prisons/
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Davis CS, Carr DH. 2017. Self-regulating profession? Administrative discipline of “pill mill” physicians in
Florida. Subst. Abuse 38(3):265–68
Degenhardt L, Conroy E, Gilmour S, Collins L. 2005a. The effect of a reduction in heroin supply in Australia
upon drug distribution and acquisitive crime. Br.J.Criminol.45:2–224
Degenhardt L, Day C, Dietze P, Pointer S, Conroy E, et al. 2005b. Effects of a sustained heroin shortage in
three Australian States. Addiction 100:908–20
Degenhardt L,Reuter P, Collins L,Hall W.2005c.Evaluating explanations of the Australian ‘heroin shortage.’
Addiction 100(4):459–69
Delcher C, Wagenaar AC, Goldberger BA, Cook RL, Maldonado-Molina MM. 2015. Abrupt decline in
oxycodone-caused mortality after implementation of Florida’s Prescription Drug Monitoring Program.
Drug Alcohol Depend. 150:63–68
D’Hotman D, Pugh J, Douglas T. 2018. When is coercive methadone therapy justied? Bioethics 32(7):405–13
Dowell D, Haegerich TM, Chou R. 2016. CDC guideline for prescribing opioids for chronic pain—United
States. JAMA 315(15):1624–45
Drucker E. 2002. Population impact of mass incarceration under New York’s Rockefeller drug laws: an analysis
of years of life lost. J. Urban Health 79(3):434–35
Drug Enforc. Adm. (DEA). 2019. National drug threat assessment. Rep. DEA-DCT-DIR-007-20, Dep.
Justice, Washington, DC. https://www.dea.gov/sites/default/les/2020-01/2019-NDTA-nal-01-
14-2020_Low_Web-DIR-007-20_2019.pdf
Dyer O. 2015. Murder trials begin in US against two high opioid prescribers. BMJ 351:h4827
Edlund MJ, Martin BC, Russo JE, DeVries A, Braden JB, Sullivan MD. 2014. The role of opioid prescription
in incident opioid abuse and dependence among individuals with chronic non-cancer pain: the role of
opioid prescription. Clin.J.Pain30(7):557–64
Engberg J, Morral AR. 2006. Reducing substance use improves adolescents’ school attendance. Addiction
101(12):1741–51
Estelle v. Gamble, 429 U.S. 97 (1976)
Evans WN, Lieber EM, Power P. 2019. How the reformulation of OxyContin ignited the heroin epidemic.
Rev. Econ. Stat. 101(1):1–15
Farabee D, Prendergast M, Anglin MD. 1998. The effectiveness of coerced treatment for drug-abusing of-
fenders. Fed. Probat. 62:3–10
Farabee D, Prendergast M, Cartier J, Wexler H, Knight K, Anglin MD. 1999. Barriers to implementing ef-
fective correctional drug treatment programs. Prison J. 79(2):150–62
Felbab-Brown V. 2019. Mexico’s out-of-control criminal market in foreign policy. Rep., Brookings, Washington,
DC. https://www.brookings.edu/wp-content/uploads/2019/03/FP_20190322_mexico_crime-2.
pdf
Forman J Jr. 2012. Racial critiques of mass incarceration: beyond the new Jim Crow. NYU Law Rev. 87:101–46
Gandossy RP, Williams JR, Cohen J, Harwood HJ. 1980. Drugs and crime: a survey and analysis of the literature.
Natl. Inst. Justice Rep. NCJ 159074, Dep. Justice, Washington, DC
Gau JM, Brooke EJ. 2017. An assessment of the impact of a multipronged approach to reducing problematic
pain clinics in Florida. J. Drug Issues 47(2):185–204
Gerstein DR, Johnson RA, Harwood HJ, Fountain D, Suter N, Malloy K. 1994. Evaluating recovery services: the
California drug and alcohol treatment assessment CalDATA general report submitted to the State of California,
Department of Alcohol and Drug Programs. Rep., Calif. Dep. Alcohol Drug Progr., Sacramento
Goldkamp JS, White MD, Robinson JB. 2001. Do drug courts work? Getting inside the drug court black box.
J. Drug Issues 31(1):27–72
Goldstein PJ. 1985. The drugs/violence nexus: a tripartite conceptual framework. J. Drug Issues 15(4):493–506
Goldstein PJ, Brownstein HH, Ryan PJ, Bellucci PA. 1989. Crack and homicide in New York City, 1988: a
conceptually based event analysis. Contemp. Drug Probl. 16(4):651–87
Green DP, Winik D. 2010. Using random judge assignments to estimate the effects of incarceration and
probation on recidivism among drug offenders. Criminology 48(2):357–87
Green TC, Clarke J, Brinkley-Rubinstein L, Marshall BDL, Alexander-Scott N, et al. 2018. Postincarcera-
tion fatal overdoses after implementing medications for addiction treatment in a statewide correctional
system. JAMA Psychiatry 75(4):405–7
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Hall W, Ward J, Mattick R. 1993. Methadone maintenance treatment in prisons: the New South Wales expe-
rience. Drug Alcohol Rev. 12(2):193–203
Hamilton Z, Campbell CM, Van Wormer J, Kigerl A, Posey B. 2016. Impact of swift and certain sanctions:
evaluation of Washington State’s policy for offenders on community supervision. Criminol. Public Policy
15:1009–72
Hammersley R, Forsyth A, Morrison V, Davies JB. 1989. The relationship between crime and opioid use.
Addiction 9:1029–43
Hawken A. 2018. Economic implications of HOPE from the demonstration eld experiment. Criminol. Public
Policy 17(4):901–6
Hawken A, Kleiman M. 2009. Managing drug involved probationers with swift and certain sanctions: evaluating
Hawaii’s HOPE. Rep. NCJ 229023, Natl. Inst. Justice, Washington, DC
Hawley M. 2002. Heroin shortage: the cause. Platypus Mag. 76:43–48
Hedrich D, Alves P, Farrel M, Stöver H, Møller L, Mayet S. 2012. The effectiveness of opioid maintenance
treatment in prison settings: a systematic review. Addiction 107(3):501–17
Hser YI, Teruya C, Brown AH, Huang D, Evans E, Anglin MD. 2007. Impact of California’s Proposition 36
on the drug treatment system: treatment capacity and displacement. Am. J. Public Health 97(1):104–9
Holloway KR, Bennett TH, Farrington DP. 2006. The effectiveness of drug treatment programs in reducing
criminal behavior: a meta-analysis. Psicothema 18(3):620–29
Humphreys K. 2017. Avoiding globalisation of the prescription opioid epidemic. Lancet 390(10093):437–39
Inciardi JA, McBride DC. 1994. Treatment Alternatives to Street Crime. Darby, PA: Diane Publ.
Inciardi JA,Surratt HL, Kurtz SP, Cicero TJ. 2007a. Mechanisms of prescription drug diversion among drug-
involved club- and street-based populations. Pain Med. 8(2):171–83
Inciardi JA,Surratt HL, Lugo Y,Cicero TJ. 2007b. The diversion of prescription opioid analgesics. Law Enforc.
Executive Forum 7(7):127–41
Jarvis BP, Holtyn AF, Subramaniam S, Tompkins DA, Oga EA, et al. 2018. Extended-release injectable nal-
trexone for opioid use disorder: a systematic review. Addiction 113(7):1188–120
Johnson BD, Goldstein PJ, Preble E, Schmeidler J,Lipton DS,et al. 1985.Taking Care of Business: The Economics
of Crime by Heroin Abusers. Lexington, MA: Lexington Books
Kaplan J. 1983. The Hardest Drug: Heroin and Public Policy. Chicago: Univ. Chicago Press
Kelly SM, O’Grady KE, Jaffe JH, Gandhi D, Schwartz RP. 2013. Improvements in outcomes in methadone
patients on probation/parole regardless of counseling early in treatment. J. Addict. Med. 7(2):133–38
Kennedy DM.2009.Deterrence and Crime Prevention: Reconsidering the Prospect of Sanction. New York: Routledge
Kennedy-Hendricks A, Richey M, McGinty EE, Stuart EA, Barry CL, Webster DW. 2016. Opioid overdose
deaths and Florida’s crackdown on pill mills. Am. J. Public Health 106(2):291–97
Kiang MV, Humphreys K, Cullen MR, Basu S. 2020. Opioid prescribing patterns among medical providers
in the United States, 2003–17: retrospective, observational study. BMJ 368:16968
Kilmer B, Nicosia N, Heaton P, Midgette G. 2013. Efcacy of frequent monitoring with swift, certain, and
modest sanctions for violations: insights from South Dakota’s 24/7 Sobriety Project. Am. J. Public Health
103(1):e37–43
Kilmer B, Reuter P. 2009. Prime numbers: doped. Foreign Policy, Oct. 16. https://foreignpolicy.com/2009/
10/16/prime-numbers-doped/
King RS, Pasquarella J. 2009. Drug courts: a review of the evidence. Rep., Sentencing Proj., Washington, DC.
https://www.sentencingproject.org/publications/drug-courts-a-review-of-the-evidence/
Klag S, O’Callaghan F, Creed P. 2005. The use of legal coercion in the treatment of substance abusers: an
overview and critical analysis of thirty years of research. Subst. Use Misuse 40(12):1777–95
Kleiman MAR. 1994. Against Excess: Drug Policy for Results. New York: Basic Books
Kleiman MAR. 2009. When Brute Force Fails: How to Have Less Crime and Less Punishment.Princeton,NJ:
Princeton Univ. Press
Kolodny A, Courtwright DT, Hwang CS, Kreiner P, Eadie JL, et al. 2015. The prescription opioid and heroin
crisis: a public health approach to an epidemic of addiction. Annu. Rev. Public Health 36:559–74
Kuchler H, Verbitsky N, Jennings T, Connaire S. 2020. Insys executives are sentenced to prison time, putting
opioid makers on notice. Financial Times.Jan.https://www.pbs.org/wgbh/frontline/article/opioid-
maker-insys-executives-sentenced-prison-subsys/
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Kuehn BM. 2014. CDC: major disparities in opioid prescribing among states: some states crack down on
excess prescribing. JAMA 312(7):684–86
Larney S, Dolan K. 2009. A literature review of international implementation of opioid substitution treatment
in prisons: equivalence of care? Eur. Addict. Res. 15(2):107–12
Lattimore PK, MacKenzie DL, Zajac G, Dawes D, Arsenault E, Tueller S. 2016. Outcome ndings from
the HOPE Demonstration Field Experiment: Is swift, certain, and fair an effective supervision strategy?
Criminol. Public Policy 15(4):1103–41
Lee JD, Nunes EV,Novo P,Bachrach K, Bailey GL, et al. 2018.Comparative effectiveness of extended-release
naltrexone versus buprenorphine-naloxone for opioid relapse prevention (X:BOT): a multicentre, open-
label, randomised controlled trial. Lancet 391(10118):309–18
Linden M, Marullo S, Bone C, Barry DT, Bell K. 2018. Prisoners as patients: the opioid epidemic, medication-
assisted treatment, and the Eighth Amendment. J. Law Med. Ethics 46(2):252–67
Longshore D, Hawken A, Urada D, Anglin MD. 2006. Evaluation of the Substance Abuse and Crime Prevention
Act: SACPA cost-analysis report (rstandsecondyears).Rep.,UCLA Integr.Subst.Abuse Progr.,Los Angeles.
http://www.uclaisap.org/prop36/documents/sacpa_costanalysis.pdf
Ludwig AS, Peters RH. 2014. Medication-assisted treatment for opioid use disorders in correctional settings:
an ethics review. Int. J. Drug Policy 25(6):1041–46
Maradiaga JA, Nahvi S, Cunningham CO, Sanchez J, Fox AD. 2016. “I kicked the hard way. I got incarcer-
ated.” Withdrawal from methadone during incarceration and subsequent aversion to medication assisted
treatments. J. Subst. Abuse Treat. 62:49–54
Marlowe DB, Merikle EP, Kirby KC, Festinger DS, McLellan AT. 2001. Multidimensional assessment of
perceived treatment-entry pressures among substance abusers. Psychol. Addict. Behav. 15(2):97–198
Mars SG, Bourgois P, Karandinos G, Montero F, Ciccarone D. 2014. “Every ‘never’ I ever said came true”:
transitions from opioid pills to heroin injecting. Int. J. Drug Policy 25(2):257–66
Marsch LA. 1998. The efcacy of methadone maintenance interventions in reducing illicit opiate use, HIV
risk behavior and criminality: a meta-analysis. Addiction 93(4):515–32
Massing M. 2000. The Fix. Berkeley: Univ. Calif. Press
Mattick RP, Breen C, Kimber J, Davoli M. 2009. Methadone maintenance therapy versus no opioid replace-
ment therapy for opioid dependence. Cochrane Database Syst. Rev. 3:CD002209
Matusow H, Dickman SL, Rich JD, Fong C, Dumont DM, et al. 2013. Medication assisted treatment in US
drug courts: results from a nationwide survey of availability, barriers and attitudes. J. Subst. Abuse Treat.
44(5):473–80
Mauer M. 2006. Race to Incarcerate. New York: New Press
McDonald R, Strang J. 2016. Are take-home naloxone programmes effective? Systematic review utilizing
application of the Bradford Hill criteria. Addiction 111(7):1177–87
Meier B. 2007. In guilty plea, Oxycontin maker to pay $600 million. New York Times, May 10. https://www.
nytimes.com/2007/05/10/business/11drug-web.html
Meier B. 2018. Pain Killer: An Empire of Deceit and the Origin of America’s Opioid Epidemic. New York: Random
House
Midgette G, Davenport S, Caulkins JP, Kilmer B. 2019. What America’s users spend on illegal drugs, 2006–2016.
Rep. RR-3140, RAND, Santa Monica, CA
Minozzi S, Amato L, Vecchi S, Davoli M, Kirchmayer U, Verster A. 2011. Oral naltrexone maintenance treat-
ment for opioid dependence. Cochrane Database Syst. Rev. 4:CD001333
Mitchell O, Wilson DB, MacKenzie DL. 2012. The effectiveness of incarceration-based drug treatment on
criminal behavior: a systematic review. Campbell Syst. Rev. 8(1):1–76
Moore MH. 1973. Policies to achieve discrimination on the effective price of heroin. Am. Econ. Rev. 63(2):270–
77
Morris N, Tonry M.1991.Between Prison and Probation: Intermediate Punishments in a Rational Sentencing System
.
New York: Oxford Univ. Press
Muhuri PK, Gfroerer JC, Davies MC. 2013. Associations of nonmedical pain reliever use and initiation of heroin use
in the United States. CBHSQ Data Rev Rep., SAMHSA, Rockville, MD
Musto DF. 1999. The American Disease: Origins of Narcotic Control. New York: Oxford Univ. Press
www.annualreviews.org
•
Opioids and the Criminal Justice System .

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Natl. Acad. Sci. Eng. Med. 2017. Pain management and the opioid epidemic: balancing societal and individual benets
and risks of prescription opioid use. Rep., Natl. Acad. Sci. Eng. Med., Washington, DC
Nicosia N, Kilmer B,Heaton P.2016. Can a criminal justice alcohol abstention programme with swift, certain,
and modest sanctions (24/7 Sobriety) reduce population mortality? A retrospective observational study.
Lancet Psychiatry 3(3):226–32
Nordstrom BR, Dackis CA. 2011. Drugs and crime. J. Psychiatry Law 39(4):663–87
Nunes EV, Shulman M. 2020. Commentary on Stein et al. (2020): Whither detoxication in the face of the
opioid epidemic? Addiction 115(1):95–96
Nunn A, Zaller N, Dickman S, Trimbur C, Nijhawan A, Rich JD. 2009. Methadone and buprenorphine
prescribing and referral practices in US prison systems: results from a nationwide survey. Drug Alcohol
Depend. 105(1–2):83–88
O’Connell DJ, Brent JJ, Visher CA. 2016. Decide your time. Criminol. Public Policy 15(4):1073–102
O’Connor S. 2017. Meth precursor chemicals from China: implications for the United States. Rep., US-China Econ.
Secur. Rev. Comm., Washington, DC. https://www.uscc.gov/sites/default/les/Research/Staff%
20Report_PrecursorChemicalReport%20071816_0.pdf
Paoli L, Greeneld VA, Reuter P. 2009. The World Heroin Market: Can Supply Be Cut? New York: Oxford Univ.
Press
Pardo B, Davis LM, Moore M. 2019a. Characterization of the synthetic opioid threat prole to inform inspection and
detection solutions. Rep., RAND, Santa Monica, CA
Pardo B, Reuter P. 2018. Narcotics and drug abuse: foreshadowing of 50 years of change. Criminol. Public Policy
17(2):419–36
Pardo B, Taylor J, Caulkins JP, Kilmer B, Reuter P, Stein BD. 2019b. The future of fentanyl and other synthetic
opioids. Rep., RAND, Santa Monica, CA
Parker RN, Nash R, Auerhahn K. 1998. Alcohol, drugs, and violence. Annu. Rev. Sociol. 24:291–311
Parmar MKB, Strang J, Choo L, Meade AM, Bird SM. 2017. Randomized controlled pilot trial of naloxone-
on-release to prevent post-prison opioid overdose deaths. Addiction 112(3):502–15
Pfaff JF. 2014. Escaping from the standard story: why the conventional wisdom on prison growth is wrong,
and where we can go from here. Fed. Sentencing Rep. 26(4):265–70
Pfaff JF. 2017. Locked In: The True Causes of Mass Incarceration and How to Achieve Real Reform. New York: Basic
Books
Poklis A. 1995. Fentanyl: a review for clinical and analytical toxicologists. J. Toxicol. Clin. Toxicol. 33(5):439–47
Pollack H, Reuter P, Sevigny EL. 2011. If drug treatment works so well, why are so many drug users in prison?
NBER Work. Pap. 16731. https://doi.org/10.3386/w16731
Pollack HA, Reuter P. 2014. Does tougher enforcement make drugs more expensive? Addiction 109(12):1959–
66
Powell D, Pacula RL, Taylor E. 2020. How increasing medical access to opioids contributes to the opioid
epidemic: evidence from Medicare Part D. J. Health Econ. 71:102286
Preble E, Casey J. 1969. Taking care of business: the heroin user’s life on the street. Int. J. Addict. 4:1–24
Prendergast ML, Podus D, Chang E, Urada D. 2002. The effectiveness of drug abuse treatment: a meta-
analysis of comparison group studies. Drug Alcohol Depend. 67(1):53–72
Pres. Comm. Law Enforc. Adm. Justice. 1967. The challenge of crime in a free society. Rep., Pres. Comm. Law
Enforc. Adm. Justice, Washington, DC
QuintilesIMS Inst. 2017. United States for non-dependence: an analysis of the impact of opioid overprescribing in
America. Rep., Pacira Biosci., Parsippany, NJ. https://www.planagainstpain.com/wp-content/
uploads/2017/09/PlanAgainstPain_USND.pdf
Reuter P. 1984. The (continued) vitality of mythical numbers. Public Interest 75:135–47
Reuter P. 2009. Systemic violence in drug markets. Crime Law Soc. Change 52(3):275–84
Reuter P, Kleiman M. 1986. Risks and prices: an economic analysis of drug enforcement. Crime Justice Annu.
Rev. Res. 7:289–340
Rigg KK, Kurtz SP, Surratt HL. 2012. Patterns of prescription medication diversion among drug dealers.
Drugs Educ. Prev. Policy 19(2):145–55
Rigg KK, March SJ, Inciardi JA. 2010. Prescription drug abuse & diversion: role of the pain clinic. J. Drug
Issues 40(3):681–701
. Caulkins et al.

CR04CH14_Caulkins ARjats.cls September 13, 2020 23:41
Rocheleau AM, Boyum D. 1994. Measuring heroin availability in three cities. Off. Natl. Drug Control Policy
Rep., Executive Off. President, Washington, DC
Simeone R. 2017. Doctor shopping behavior and the diversion of prescription opioids. Subst. Abuse Res. Treat.
11:1178221817696077
Smithson M, McFadden M, Mwesigye S, Casey T. 2004. The impact of illicit drug supply reduction on health
and social outcomes: the heroin shortage in the Australian Capital Territory. Addiction 98:340–48
Spohn C, Holleran D. 2002. The effect of imprisonment on recidivism rates of felony offenders: a focus on
drug offenders. Criminology 40(2):329–58
Sporer KA, Firestone J, Isaacs SM. 1996. Out-of-hospital treatment of opioid overdoses in an urban setting.
Acad. Emerg. Med. 3(7):660–67
Springer SA, Altice FL, Brown SE, Di Paola A. 2015. Correlates of retention on extended-release naltrex-
one among persons living with HIV infection transitioning to the community from the criminal justice
system. Drug Alcohol Depend. 157:158–65
Stallwitz A, Stöver H. 2007. The impact of substitution treatment in prisons: a literature review. Int. J. Drug
Policy 18(6):464–74
Stein M, Herman D, Conti M, Anderson B, Bailey G. 2020. Initiating buprenorphine treatment for opioid use
disorder during short-term in-patient ‘detoxication’: a randomized clinical trial. Addiction 115(1):82–94
Sufrin C, Sutherland L, Beal L, Terplan M, Latkin C, Clarke JG. 2020. Opioid use disorder incidence and
treatment among incarcerated pregnant people in the US: results from a national surveillance study.
Addiction. https://doi.org/10.1111/add.15030
Surratt HL,O’Grady C, Kurtz SP,Stivers Y,Cicero TJ,et al. 2014. Reductions in prescription opioid diversion
following recent legislative interventions in Florida. Pharmacoepidemiol. Drug Saf. 23:314–20
Tanum L, Solli KK, Latif ZE, Benth JŠ, Opheim A, et al. 2017. Effectiveness of injectable extended-release
naltrexone versus daily buprenorphine-naloxone for opioid dependence: a randomized clinical noninfe-
riority trial. JAMA Psychiatry 74(12):1197–205
Travis J, Western B, Redburn FS. 2014. The Growth of Incarceration in the United States: Exploring Causes and
Consequences. Washington, DC: Natl. Acad. Press
Wakeman SE. 2017. Why it’s inappropriate not to treat incarcerated patients with opioid agonist therapy.
AMA J. Ethics 19(9):922–93
Warren E, Viney R, Shearer J, Shanahan M, Wodak A, Dolan K. 2006. Value for money in drug treatment:
economic evaluation of prison methadone. Drug Alcohol Depend. 84(2):160–66
Weisburd D, Braga AA. 2006. Introduction: understanding police innovation. In Police Innovation: Contrasting
Perspectives, ed. D Weisburd, AA Braga, pp 1–23. Cambridge, UK: Cambridge Univ. Press
Werb D, Kamarulzaman A, Meacham M, Rafful C, Fisher B, et al. 2016. The effectiveness of compulsory drug
treatment: a systematic review. Int. J. Drug Policy 28:1–9
Wilson N, Kariisa M, Seth P, et al. 2020. Drug and opioid-involved overdose deaths—United States, 2017–
2018. Morb. Mortal. Wkly. Rep. 69:290–97
Wood E, Stoltz JA, Li K, Montaner JSG, Kerr T. 2006. Changes in Canadian heroin supply coinciding with
the Australian heroin shortage. Addiction 101(5):689–95
Zeng Z. 2019. Jail inmates in 2017. Bur. Justice Stat. Rep. NCJ 251774, Dep. Justice, Washington, DC. https://
www.bjs.gov/content/pub/pdf/ji17.pdf
www.annualreviews.org
•
Opioids and the Criminal Justice System .
